I know it sounds superfluous, extreme or incredulous, and hyperbolic but at this point, maybe it’s best to stretch the boundaries of logical reasoning or science – what is demonstrate-able or reproducible provided all conditions are kept constant.
For a second, let’s say we push the logic into a black hole and focus on animism – a system many Africans are well-accustomed to. For any acculturated African, when there is a mishap such as the death of a loved one particularly a newborn, we often make remarks like “God gives, God takes”. We say this in spite of other likelihoods such as stress, lack of essential medicines or a simple first aid kit to stop excess bleeding during child delivery, interconnections between malnourishment of expectant mothers in the gestational period and how it affects the physiological functions of newborns.
We often don’t realize how upstream determinants of health such as low economic outcomes and the lack of access to economic opportunities, long distances between residential areas and the nearest community health centres, all serve as a self-fulfilling prophesy? Even if the hospitals are within reach, aren’t a lot of women and girls fated to lose their babies or worse their lives due to a lack of capacity of the health workforce or poor supply of equipment to carry out quick diagnosis of a possible cardiovascular issue, HIV or hormonal derangement.
When one thinks about how indigenous communities see the birth of a child in Africa, it makes complete sense. Among the Yoruba tribe like other African societies, as a form of greeting, well-wishers say to the new mothers “eku ewu omo”, thus, congratulating the women for making it out of the delivery room in spite of the risk associated with the birthing procedure. For friends and family, the psychological distress of carrying child to term pales in comparison to the risk of a birth operation. Yet for a lot of families in Africa, the activities culminating into a nine-month journey, such as expectant mothers adhering to all traditional health information during pregnancy, looking to the supernatural, shopping for the unborn baby, and choosing a name could quickly become a futile exercise in a few second.
Maternal mortality: witchcraft or a bewitched system is like a fable. A proverbial tale of a haunted house. In the story, every young woman walks into the house with a dream to find a treasure. However, to their tragic end, they never quite reach the treasure. Worse, there is a high livelihood that they may lose their lives. The treasure is the baby. The haunted house is the entire health system.
In Nigeria, it is common knowledge that more women die each year from complications of pregnancy and child birth than anywhere else in Africa. According to the Nigeria Health Watch in a MSD for Mothers report (2022), Nigeria has one of the highest maternal mortality ratio ranking fourth globally and accounting for one-fifth of maternal death across the world. Some of the leading causes is depicted below.
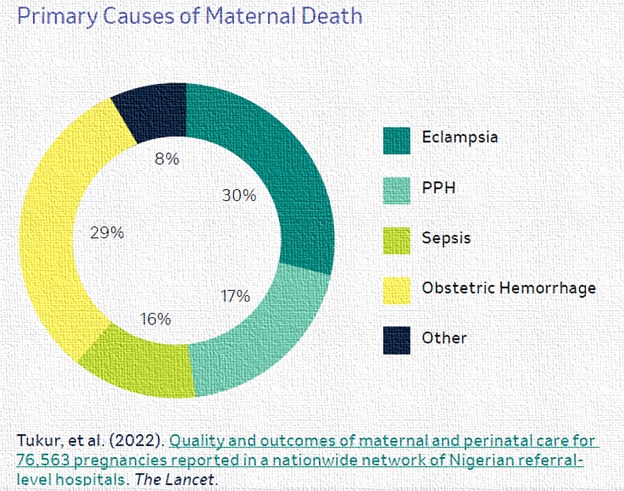
Source: MSD for Mothers (Evidence for Impact 2022).
So why are we losing young, productive women from the far end of the Global South in Pakistan to the deeper South of Nigeria at such alarming rate? The answer lies in the title of my fable: Witchcraft or A Bewitched health system.
Less than three years ago, a group of researchers conceptualized a community-informed maternal death review to look into the conditions that led to pregnant women dying in countries and to pilot a community accountability mechanism for maternal death.
The study which was conducted across all the geopolitical zones in Nigeria found that pregnant women in the South side were more likely to die due to shortfalls in the strength and capacity of the health workforce (including the traditional birth attendants, TBAs), perception that only women with complications need to visit a health facility, negative attitude of health workers towards patients and low health-seeking behavior associated with widespread reliance on religious beliefs. High mortality among women from the Northern parts of Nigeria was associated with patriarchy which places the decision to use health centre on husbands and other male figures. Another group of traditional custodians against the agency of women over their reproductive health were found to be mothers and mothers-in-law, according to the 2022 MSD for Mothers report. These groups constituted some of the most significant actors to address maternal health in sub-Saharan Africa. More on the study findings on maternal health in Nigeria are outlined below.
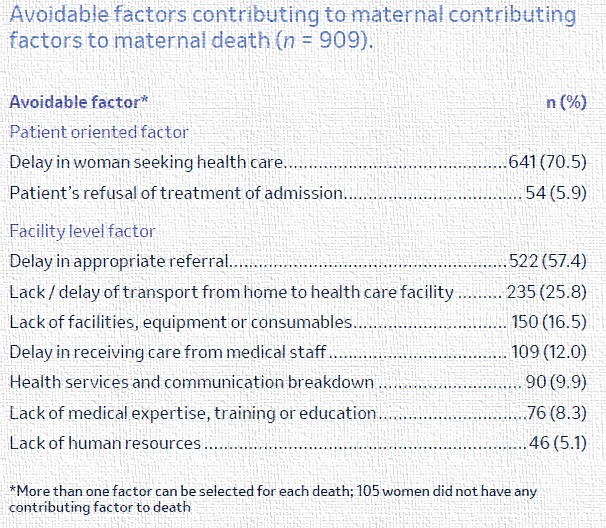
Source: MSD for Mothers (Evidence for Impact 2022)
Alluding the failure to adequately address the roots of maternal death by blaming it on an X-factor makes death caused by man’s inhumanity appear like the proverbial ‘hand of God’. On the other hand, consigning the challenge of the death of mothers to a bewitched or (bedeviled) health system, resembles a case of learned helplessness. Whether you support the former or later argument, one thing we are realizing is traditional actors such as decision-makers need to employ more innovative evidence-informed models that considers the contribution of other groups such as non-State actors – community leaders, faith-based organizations.
Judging by the barriers to maternal health earlier outlined, experts from MSD for Mothers recommend that:
- State government commit to building socio-cultural structures that consider the indigenous people (including community leadership). Such efforts will accelerate accountability for maternal death at grass root level. It will also make advocacy for the adoption of safe practice in maternal healthcare more effective.
- Engagement of TBAs, being trusted members of host communities is crucial. This workforce must be adequately empowered in skills and knowledge to identify danger signs in pregnancy and refer women to health facilities.
- There’s need to employ evidence-based approaches in health messaging from health providers and the media industry to the general public. One that support women to make better health-seeking decision, which will lead to better maternal health outcomes
In sum, there is an urgent need for these actors to embrace a whole government-, whole society approach, not just for the next 8 years according to the 2030 UN SDG target, but think long-term solutions.
As a members of various African societies, we must be willing to look far and wide, to end this vicious cycle for the sake of our daughters and sisters. Let us embrace the positive lessons of history and quickly chart a different course, particularly when the solutions we seek have been demonstrated in other global communities. We can agree collectively to transform the haunted house into a safe haven for mothers, newborns and everyone.